ARTICLES
षारीरिक विकलांगता एक अभिषाप नहीं है।
सेरेब्रल पालिसी का इलाज अब सम्भव है।
नवजात षिषु में मस्तिष्क के क्षतिग्रस्त हो जाने की वजह से होने वाली षारीरिक एवं मानसिक विकलांगता जैसी बीमारी के समुह को सेरेब्रल पालिसी के नाम से जाना जाता है। आजकल पोलियो उन्मूलन र्कायक्रम की वजह से पोलियों से ग्रसित होने वाले बच्चों की संख्या लगातार कम होती जा रही है। वही अच्छी चिकित्सिय सुविधाओ के उपलब्ध होने की वजह से कम उम्र में पैदा हुए नवजात षिषु को बचाने में बहुत अधिक सफलता मिल रही है परन्तु उनके अविकसित मस्तिष्क पर पड़ने वाले दुश्परिणाम के कारण सेरेब्रल पालिसी से ग्रसित होने वाले बच्चो की संख्या लगातार बढ़ती जा रही है, और अब यह बच्चों में होने वाली षारीरिक विकलंागता का एक प्रमुख कारण बन गयी है। यह बीमारी बच्चों में जन्म के समय से 2) वर्श की उम्र तक मष्तिश्क के कुछ भागो के क्षतिग्रस्त हो जाने से होता है। यह बीमारी कम वजन एवं समय से पहले पैदा होने वाले बच्चों में बहुत ज्यादा होने की संभावना होती है।
इनके प्रमुख कारणों में नवजात षिषु को जन्म के समय सॉस में रूकावट, तेज पीलिया, मस्तिष्क ज्वर एवं मस्तिष्क में चोट लगने और गर्भ के समय मॉ को झटके आने या किसी हानिकारक दवाओं की वजह से होता है। जिसकी वजह से नवजात षिषु अपनी क्रिया कलाप को ठीक समय पर षुरूआत न करके या तो देर से षुरू करते है या नहीं कर पाते है। एवं बच्चा चलने,उठने, बैठने में या तो पूरी तरह से असमर्थ होता है या परेषानी महसूस करता है। इसके अलावा इन बच्चों में कुछ अन्य परेषानियॉ भी होती है जिनमें दौरे का पड़ना, बुद्धि का विकास न होना, बोलने,सुनने दखने की समस्या के साथ-साथ षरीर में बीमारी रोद्यक षक्तियो का कम होना जिसकी वजह से इन बच्चों को समय-समय पर बुखार खॉसी बलगम और अन्य बाीमारियॉ होती रहती है।
पिछले कुछ सालों पहलें तक ऐसी भयावह बीमारी का इलाज सम्भव नहीं था, और इन बच्चों के माता-पिता इलाज के खोज मे निरन्तर इधर-उधर भटकते रहते थें और अन्त में असहाय होकर के इनकी षारीरिक परेषानियों को एक अभिषाप मानकर के इलाज कराना बन्द कर देते थें। और ऐसे बच्चे जीवन पर्यन्त विंकलांग ही रह जाते थें। परन्तु आजकल की अत्याधुनिक चिकित्सीय विकास की वजह से अब इन बच्चों को वापस अपने पैरों पर खड़ा करके समाज की मुख्य धारा से जोड़ने में सफलता मिल रही है। जो कि इन विषिश्ठ बच्चों एवं उनके मॉ-बॉप के लिए चमत्कार से कम नहीं होता है।
इस बीमारी का इलाज जितनी कम उम्र में षुरू किया जाता है उतनी अधिक सफलता मिलती है। इस बीमारी के षुरूवाती दौर में पहचान के लक्षण निम्न है- जैसे कि समय से पहले पैदा हुए बच्चें, एवं 1ण्5 से कम वजन वाले बच्चों में, जन्म के समय बच्चे का न रोना, मॉ के दूध को न लेना, तेज पीलिया, गर्दन रोकने, बैठने एवं खड़े होने में अक्षमता, हाथ-पैरो का सुचारू रूप से उपयोग न करना, मुॅह से लार का टपकना, हाथ-पैर की मॉसपेषियो का बहुत सख्त एवं एकदम ढीला होने के साथ-साथ बोलने,सुनने,देखने,एवं समझने में अक्षमता एवं दौरा पड़ना जैसे प्रमुख लक्षण होते है, इनमें से कुछ लक्षणों के पाए जाने पर बच्चों का इलाज बहुत ही जल्द षुरू कर दिया जाए तो ढीक होने की सम्भावना बहुत ही ज्यादा रहती है। इस बीमारी में कई तरह के लक्षण दिखाई पड़ते है जैसे की कुछ बच्चों के हाथ-पैर कि मॉषपेषियॉ बहुत सख्त होती है या तो ढीली होती है। इस बीमारी के अन्य लक्षणों में हाथ-पैरों को बिना किसी उद्देष्य के घुमाते रहना एवं षरीर का सन्तुलन न बन पाना है। यह बीमारी षरीर के किसी एक अंग से लेकर के पूरे षरीर को प्रभावित कर सकती है। इस बीमारी की पूरी जानकारी बच्चों के हाव-भाव देखने और षारीरिक परिक्षण के तदुपरान्त होता है। इस बीमारी में डत्प् एवं ब्ण्ज्ण् ैबंद जैसी जॉचो की जरूरत बहुत कम पड़ती है। इस बीमारी से ग्रसित होने वालो बच्चों की षारीरिक विकलांगता तो बहुत कम होती है, जिसमें उनको सामान्य रूप से पहचानना कठिन होता है एवं कुछ बच्चों में बहुत ज्यादा होती है जिसकी वजह से वह अपनी दिनचर्या बिलकुल नहीं कर पाते है।
इस बीमारी के इलाज में हमारा मुख्य उद्देष्य बच्चों की षारीरिक विकलांगता को दूर करना एवं उनके षारीरिक एवं मानसिक क्षमता को बढ़ाना है, जिससे कि वह समाज में अपनी दिनचर्या सुचारू रूप से कर सके। इन बच्चों में षारीरिक विकलांगता के साथ-साथ सम्बन्धित विकारो का इलाज षुरूआती दौर में कर देने से आजकल नई-नई तकनीकिया विकसित हुई है, जिसमें कि न्यूरोडवलपमेन्टल थेरेपी,सेन्सरी इन्टीग्रेसन, मॉसपेषियो को मजबूत करने वाली कसरतो का प्रमुख महत्व है। इसके अलावा सख्त हुई मॉसपेषियों को ढीला करने के लिए बाटुलियन टाक्सिन,प्लास्टर एवं जापानी सर्जिकल तकनीकी वेेबे का एक प्रमुख स्थान है, जिसकी वजह से बच्चों में कसरत कराना आसान हो जाता है, एवं ऐसे बच्चे बहुत तेजी से विकास करने लगते है। आजकल इन सभी तकनीको का एक साथ प्रयोग करके चमत्कारिक परिणाम देखा गया है। नयूरोडवलपमेन्टल थिरेपी में बच्चो को उनके सामान्य षारीरिक विकास के आधार पर कसरत एवं टेªनिग दी जाती है एवं सेन्सरी इन्टीग्रेसन जैसी तकनीकी से तमाम तरह की ेजपउनसंजपवद दिये जाते है, जिससे कि इन बच्चों में सर्वागीण विकास हो। इन बच्चों के षरीर में कुछ मॉसपेषियॉ कमजोर होती है, जिसके अगर मजबूती प्रदान कर दी जाय तो बच्चा अपनी दिनचर्या सामान्य रूप से कर सकता है। 2 से 5 वर्श के बच्चों में सख्तपन को कम करने के लिए बाटुलिनम टॉक्सिन इन्जेक्सन का उपयोग किया जाता है। यह इन्जेक्सन सख्त हुई मॉसपेषियो में लगाया जाता है जिससे कि उनके सख्तपन कम हो जाता है जिसकी वजह से बच्चे कसरत आसानी से करा लेते है। एवं उनका षारीरिक विकास बहुत तेजी से होने लगता है। इस बाटुलिनम टाक्सिन का प्रभाव केवल 4 से 6 माह तक ही रहता है, परन्तु कसरत सही तरीके से कराते रहने से दुबारा इन्जेक्सन की जरूरत बहुत कम होती है। इसके अलावा मॉसपेषियों में सख्तपन ज्यादा होने पर कई बार प्लास्टर लगाने की जरूरत होती है परन्तु इसका प्रभाव बहुत कम समय तक रहने की वजह से इस पद्धति का उपयोग बहुत कम किया जाता है एवं आजकल वेेबे जैसी जापानी तकनीकी की वजह से बड़े बच्चों में सख्तपन को दूर करने के साथ-साथ उनकी षारीरिक क्षमता को बढ़ाने में अप्रत्याषित परिणाम देखें गए है। इस सर्जिकल तकनीकी में केवल सख्तपन से प्रभावित मॉसपेषियों का विभिन्न प्रकार की तकनीको से आपरेषन किया जाता है, जिनकी वजह से दूसरी सामान्य मॉसपेषियों की क्रियाषाीलता बनी रहती है एवं उनकी कार्यक्षमता बढ़ जाती है, जिसकी वजह से इन बच्चों में सख्तपन को दूर करने के साथ-साथ मॉषपेषियो को बहुत तेजी से मजबूती प्रदान की जा सकती है, जिससे कि इन बच्चों की क्रियाषाीलता सामान्य बच्चों की तरह होने की सम्भावना बहुत अधिक रहती है। इन तकनीकी की वजह से पूरी तरह से असहाय हो चुके बच्चों को भी उनके अपने पैरो पर खड़ा करने में सफलता मिल रहीं है एवं पिछले कुछ सालों के परिणाम स्वरूप अभी तक किसी तरह का कोई भी दुश्परिणाम नहीं देखा गया है। जो कि पहले की जाने वाली आर्थोपेडिक सर्जरी से मिलता था।.
आने वाले समय में इस वेेबे तकनीकी से हमारे बहुत सारे असहाय हो चुके बच्चों को भी सामान्य बनाने में सफलता मिलेगी। अब यह माना जाता है कि इस तरह के बच्चो का इलाज जितना जल्दी षुरू कर दिया जाय उतना ही अच्छा परिणाम देखने को मिलता है।
डा0 जितेन्द्र कुमार जैन
बाल अस्थि रोग विषेशज्ञ
त्रिषला आर्थोपेडिक क्लीनिक
एवं सेक्रेटरी,संवेदना
इलाहाबाद
मो0 – 9415235159
Email: jjain99@rediffmail.com
Role of SEMLS and OSSCS in Management of Cerebral Palsy
Phone No. – 9415235159, 0532-2468989
Email: jjain999@gmail.com
www.samvednatrust.com/
Whenever, a child is diagnosed as having cerebral palsy, the idea which comes to our mind that he is suffering from permanent brain damage and will be permanently disabled for life. Until now, it was believed that in the absence of effective treatment these children can not do their daily activity on their own for whole life and they have to be dependent on others and it was also thought that their life expectancy will be short. Most of the time parents used to wander from pillar to post in the hope of best advice and treatment and clinicians are always in dilemma regarding unpredictable out come.
But truth is far away from this belief. These children can survive up-to the age of normal person with good quality of life if they are given good treatment by multimodal approach. It is also seen that quality of life & life expectancy depends more on ambulatory capability & other associated problems: so if child can be made ambulatory & their associated medical problems tackled in timely, their life expectancy can be improved a lot. Recently, due to new concept of SEMLS & OSSCS, most of our children with cerebral palsy can be given good quality of ambulatory life with little assistive devices so that they can be better mingled in society and their capabilities are utilized in a much better way.
Disability – Apart from physical disability child can have lot of other medical problems like, Convulsive disorders , Feeding problems, Mental retardation, Constipation, Visual defects, Dental defects, Hearing defects, Sensory defects, Sleeping disorders, Speech impairment, Poor immunity, Growth retardation, Obesity, Behavior problems, Malnourishment, Perceptual problems etc.
Life expectancy & Prognosis – Survival of children in cerebral palsy is lesser than normal population due to associated disabilities; not because of cerebral palsy itself. It has also been seen that child with ambulatory capability with or without any walking aids has more survival and good quality of life than child on wheel chair.
Severely affected quadriplegic children if not managed at early age, they are not going to survive more than 30 years, on the other hand partially affected Tri & Di Plegic children can survive up to life expectancy of normal population. Now with advancement in treatment modality, life span of quadriplegic children can also be prolonged. These persons can have job, live independently, marry have children & retire, and can be active, productive members of their communities. Approximately 85% of partially involved children have the potential to become independent ambulators.
Scenario in Developing Countries – in spite of increase in life expectancy of children with cerebral palsy in developed countries, children with cerebral palsy in developing countries still have poor prognosis because of ignorance and lesser facilities of advance modality of treatment & absence of standard treatment guideline. As a result the families are confused as to what is the best for their child & the child is afraid of going anywhere, and ultimately child remains disable for whole life.
Aims & Principles of Management: We don’t have any permanent cure of cerebral palsy as brain damage can not be repaired. Aim of treatment is to increase the patient’s assets as much as possible & minimize his deficit. With proper management, we can diminish the functional impairment up to a great extent in most of the children. Regardless of their mental capacity, almost all patients can be taught something about self-care, mobility and communication. Treatment should focus on child’s ability, not disability and method should be evolved to enhance utilization of their ability. Although we can not do much in these children by managing one problem at a time, but by multimodal approach, in which their physical disability along with other associated problem can be tackled, they can be given maximum benefit. It has been seen that with improvement in their physical condition, children also improve a lot in their cognition and their personality.
Multimodal Approach – In this approach we use all available proven interventional modality in a suitable combination to prevent permanent consequences in body and decompensated changes in joint and if it happen then it should be treated early so that child can be given a good chance of recovery without loosing important phase of life. It requires multidisciplinary approach & training of parents in ADL & home based therapy programme.
Early intervention – More than 80% children with cerebral palsy can have nearly normal life with early intervention despite different grade of severity. Treatment can be started from NICU itself in high risk children with proper handling and sensory motor management. During discharge from NICU, counseling of parents can be done so that proper therapy can be started from three months onwards.
Physiotherapy – Therapy is the main stay of treatment in cerebral palsy. Traditional methods are stretching exercise, joint mobilization, electric stimulation etc. Advanced modality includes Sensory integration, Neuro-developmental therapy, Constrained Induced Movement Therapy, Strength training exercise, Horse riding, Hydrotherapy. With advance modality of therapy and early intervention, child can be given maximum benefits. Light weight polypropylene braces and walking aid is the essential part of multimodal approach & it makes the activity of daily living easier for children with cerebral palsy. Heavy weight caliper have no role in management of cerebral palsy.
Botulinum Toxin – It causes temporary and reversible blockade of cholinergic transmission at neuromuscular junction. Its effect last for only 3 to 4 months but the duration of response can be prolonged up to some extent by use of serial cast, day night splint & good physiotherapy. It is effective only in children with spastic CP and best response is seen between 2-6 years age group. It is not very effective in elder children with contracture.
Orthopedic Surgical Intervention: Contracture and bony deformities are almost inevitable in a growing child with spastic cerebral palsy and need surgical intervention at proper time to prevent joint de-compensation and over-lengthening of tendon. Now surgery is being considered an important incident in total management of patient with spastic cerebral palsy.
Routine Orthopedic Surgery – Orthopedic surgery is typically recommended when fixed deformities results in stalled motor progress, development of pain, orthotic intolerance & difficulties with care. Orthopedic surgery primarily involves fractional lengthening and tenotomy, muscle transfers, joint reconstruction, bone fusions, or bone realignment. Routinely surgery is being performed at single or two levels (eq. TA lengthening &/or adductor tenotomy) at a time and patients require repeated surgery. Routine orthopedic surgery is advised after 10-12 year age, when permanent damage to extremity is already fixed.
Problem with Routine concept– Selective control of spasticity is not possible with routine orthopedic concept and child is always left out with deformity despite repeated surgeries. Also this type of surgical intervention is not helpful in severely affected patient. Some times child develop reveres deformity (Genu Recurvatum & Crouch Gait) and ambulatory children become non-ambulatory leading to psychological upset to parents & children.
RECENT ADVANCEMENT
Single Event Multilevel Surgery (SEMLS) – Cerebral palsy is caused by sectoral or global brain damage so depending upon extent of lesion, whole of the affected limb is involved and on the other hand a single gait pattern require coordination of more than 30 muscles, so to correct gait pathology it is mandatory to balance each of the affected muscles. Child can get best result if all abnormalities are detected before surgery & corrected in single setting surgery followed by well structured therapy programme.
Early Surgical Intervention – Development of walking skill is completed by the age of five years, so 6-10 year age is ideal for surgery but it can be done at any age group. Surgery should not be delayed to long, otherwise progressive deformity and co-spasticity of muscles will lead to de-compensated changes in joint & bone. Child can develop lots of nonreversible problem with late surgical intervention like over lengthening of tendon (Tendo Achilles, Patellar tendon), development of non correctable deformity like genu recurvatum, crouch gait, bony torsion, joint dislocation, mid foot break & development of plano-valgus feet and early degenerative changes in joints, some time permanent neglect of hand function. Surgery should also be not done too early unless otherwise the child develops some joint pathology like joint dislocation & bony torsion. Surgery at properly selected age group shortens the period of therapy & with early surgical intervention child can have early schooling, early & fast rehabilitation and better extracurricular activity.
Orthopedic Selective Spasticity Control Surgery (OSSCS) – This concept is given by Dr. Takashi Matsua from Japan. It has brought a new concept in management of cerebral palsy.
Basic Concept of OSSCS – Muscles of the vertebrate body are divide into two groups according to spanning number of joints. Their functional nature differs according to their biarticular/mono-articular representation. These muscles are distributed side by side in body. Long multi-articular muscle has more propensity of spasticity & more responsible for abnormal hypertonic posture, on the other hand short mono articular muscles have more antigravity and voluntary activity & provide stability to body during antigravity posture. Selective lengthening of multi-articular muscles & preservation of mono-articular muscles (Selective Spasticity control) at all affected body parts in single setting surgery (SEMLS) lead to good balance of muscle tone in whole body. Selective spasticity control may allow many patients with CP to use motor control more effectively and functionally. With simultaneous release of spastic or athetotic multi articular agonist & antagonistic muscle in each joint of the body, the abnormal postural reflexes can be relieved along with better facilitation of reciprocal and alternate movements. This concept of surgical interval give excellent response if surgery is being carried out between 6 upto 10 year age, although it can be done at any age group after that.
BASIC DIFFERENCE BETWEEN ROUTINE ORTHOPAEDIC SURGERY AND OSSCS
|
ROUTINE ORTHOPAEDIC SURGERY |
OSSCS |
|
Complete section of tendon (no consideration of muscle behavior) |
Selective lengthening of biarticular muscle and sparing of mono articular muscle |
|
Tendon transfer |
Not done |
|
Not able to balance muscle power of antagonist |
Possible with this procedure |
|
Some time patient deteriorate |
No deterioration |
|
Usually delayed & done at the age of 9-10 year |
Early intervention from 6 year onward to prevent Joint malfunctioning |
Advantage of New Technique – Permanent correction of deformity can be achieved with this concept & recurrence is very –very rare so most of time child do not require second surgical intervention. Earlier thought was that, result of surgery in cerebral palsy is unpredictable, some feel better and some worse following surgery. Now with the advance technique and well planned surgery, child always get good outcome. Well performed surgery on properly selected patient give good result provided the rehabilitation after surgery is carefully managed. Gait pattern become much more normal with properly performed Single event multilevel surgery. Successful surgery give all round acceleration of other function like learning, speech, behavior along with motor function recovery .
Conclusion – Latest advancement in therapeutic & surgical management of cerebral palsy has given new hope for most neglected problem of human being and now they can be intergraded in main stream of society. Early intervention by the advance modality of therapeutic technique and early surgical intervention in properly selected patient always gives good functional outcome. Concept of SEMLS & OSSCS surgical concept has become a boon for these children. With improvement in physical disability, children always show excellent response in extracurricular activities & other associated medical problem.
References:-
- Gough M, Eve L C, Robinson R O, Shortland A P. Short-term outcome of multilevel surgical intervention in spastic diplegic cerebral palsy compared with the natural history. Developmental Medicine & Child Neurology 2004, 46: 91–97
- Gough. M, Schneider P, Shortland A P. The outcome of surgical intervention for early deformity in young ambulant children with bilateral spastic cerebral palsyJ Bone Joint Surg [Br] 2008;90-B:946-51
- Graham H. K,. Harvey A,. Assessment of mobility after multi-level surgery for cerebral palsy. J Bone Joint Surg [Br]2007; 89-B:993-4.
- Izumi K, et all. Effectiveness of elective muscle release surgery for children with cerebral palsy: longitudinal and stratified analysis. Developmental Medicine & Child Neurology 2004, 46: 540–547
- Maria S et al .Recovery of muscle strnegth gollowing SEMLS in diplegic spastic cerebral palsy .gait posture 26(2007)475-481
- Matsua T : cerebral palsy : Spasticity Control & Orthopaedic. An introduction to orthopaedic selective Spasticity control surgery. soufusha 2002,Tokyo.
- Mohanty, R N, Avadhani B R.Early Surgical Intervention to Facilitate Ambulatory Potential in the Rehabilitation of Spastic Diplegics . IJPMR 12, April 2001; 7-10.
- Prakash H, Ganesh T, Bhattachar S. Effect of Single Event Multilevel Soft Tissue Surgery on Gait Parameters in Spastic Diplegia. IJPMR April 2007; 18 (1): 3-6
- Smitherman J A. Tanner J R S, Hardin J W, Wagner L V, Peace L C. Mary, Gidewall A. Functional outcome following SEMLS of upper extremity in hemiplegics CP. JBJS (Am) 2011,93, 655-961.
- Thamkunanon V. Improvement of ambulatory function with multilevel soft tissue surgery in children with spastic diplegic cerebral palsy. J Med Assoc Thai. 2011 Aug; 94 Suppl 3:S183-8.
- Thomason P, Baker RJ, Dodd K, Taylor N, Selber P, Wolfe R and Graham H. Single-event multilevel surgery in children with spastic diplegia : a pilot randomised controlled trial.2011, JBJS, 93 (5) , pp. 451-460.
Paediatric Orthopedic Problem Congenital Talipus Eequino Varus (Club Foot)
Clubfoot is the most common deformity of the bones and joints in newborns. It occurs in about 1 in 1,000 babies. The cause of clubfoot is not exactly known, but it is most likely a genetic disorder. It can present as unilateral or bilateral problem. When treated by an expert in this field, will have a normal looking foot with essentially normal function. The well-treated clubfoot causes no handicap and the individual is fully able to live a normal active life. Diagnosis of CTEV can be made just by looking at the foot.
Dr Ponsetty explains use of abduction brace to parents of child with CTEV.
Treatment of CTEV starts just after birth. It is better to start treatment early as possible in first week of birth because of more strechibility of ligament and soft tissue on medial aspect of foot. Usually child requires 5-6 time of manipulation & thereafter plasters application for 1 weak to 10 days every time. After application of 5-6 plaster application percutaneous TA tenotomy is required in most of the cases followed by plaster for 1 month. Ponsetty gave new concept of manipulation and plaster application. In this technique first time elevation of first metatarsal head followed by manipulation in progressive abduction till 70 degree of abduction then correction of equines deformity by TA Tenotomy. Now most of the foot deformity in CTEV can be corrected in much better way. till few year back, most of time this deformity required corrective surgery that was mutilating and foot never became normal & flexible and recurrence rates was very much high. With the use of Ponsetty technique of manipulation & plaster application, even residual & neglected cases of CTEV in elder children can be corrected except minor surgical intervention & corrected foot always remain supple & flexible.
After successful correction, it is very important to wear CTEV shoes with abduction bar till the age of 1 year. It should be minimum for 20 hour a day followed by day time shoes along with night time wear of abduction brace for 6 month. While kicking in the foot abduction brace full time, the baby strengthens the Peroneal muscles and foot extensor muscles that counteract the pull of the Tibialis and Gastrosoleus muscles. Relapses are rare with the continued use of the foot abduction brace.It is my experience that result became much better if parents advised for exercise in the form of passive dorsiflexion of foot with pulling heal planter ward, stimulation of lateral aspect of foot so that child dorsiflexed with version actively.
Sequential change in shape of foot after successive manipulation
 |
 |
| Case of B/L CTEV | After successful correction of deformity |

Child of CTEV with abduction bar
Congenital Dislocation of Hip (CDH)
Congenital dislocation or subluxation of the hip also known as congenital acetabular dysplasia & developmental dysplasia of hip (DDH). it signify a complete or partial displacement of the femoral head out of the acetabulum or some time only dysplastic changes in acetabulam. A broader definition of DDH is simply abnormal growth of the hip. Abnormal development of the hip includes the osseous structures, such as the acetabulum and the proximal femur, and the labrum, capsule, and other soft tissues. At the time of birth 1% hip are subluxatable. But with passage of time most of the hip became stable in infancy leaving only 0.2% with residual hip instability. Usually present unilaterally. First new born child with breech presentation, female gender and with family history are more prone to have this problem. It can present as dysplasia, subluxation, classic dislocation and some time uneducable dislocation (teratogenic).
Early identification of CDH in infancy can be done by Ortolany /Barlow maneuver. In ortoloni test The examiner’s thumb is placed over the patient’s inner thigh, and the index finger is gently placed over the greater trochanter. The hip is abducted, and gentle pressure is placed over the greater trochanter. In the presence of DDH, a clunk, similar to turning a light switch on or off, is felt when the hip is reduced. Barlow described another test for DDH that is performed with the hips in an adducted position, in which slight gentle posterior pressure is applied to the hips. A clunk should be felt as the hip subluxate out of the acetabulum. But this is possible only in early infancy upto 3 month of birth after that it my be negative then child present different set of sign & symptom like of shortening of leg, gluteal fold, decrease abduction, palpable femoral head in Gluteal area.
Diagnosis can be confirmed by dynamic ultrasound and x-ray. Evaluation by ultrasound require experience in musculoskeletal ultrasonography. ultrasonologist can also assess reducibility of joint. By x-ray we can see position of femoral head and different angle & lines at the hip joint .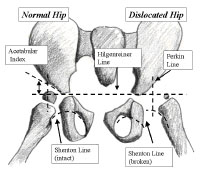
Management of child with DDH dependent upon age of presentation. We can start the treatment after 1 weak of birth. If the hip is easily dislocatable then we can ask to wear heavy diaper for few initial days if it is not helping then pavlik harness can be advised to child but its use is only applicable upto 6 month af age after that it is not going to effective. Proper application of pavlik harness is very important otherwise some it may lead to avascular necrosis of femoral head. The important aspects in the use of the harness include: ( I ) appropriate indications, (2) adequate hip flexion in the harness as verified by roentgenograms, (3) use of a good-quality harness, (4) confirmation of concentric reduction after three weeks of harness use, (5) maintenance of the patient in the harness until a normal clinical and roentgenographic examination is achieved, and (6) education of the parents.
Reducibilty of femoral head should be checked at regular interval by ultrasonic examination and x-ray. If joint is not reducible then pavlik harness should not be used and child my require adductor tenotomy and spica application. Reduction can be checked by arthrogram.
If child present in more than 1 year of age then they will require open reduction and spica application. if there is acetabular dysphasia then they will also require acetabular reorientation osteotomy . in children of more than 18 month child require open reduction along with femoral shortening and acetabular osteotomy. Early the treatment better is the result.
Post Polio Residual Paralysis
Now days with success of polio vaccination programme. New cases of post polio residual paralysis are becoming rare but society still have children & adult who have weakness & deformity of limbs due to polio. Patient with polio have lots of capability that can be enhanced if their deformity and weakness of muscle can be minimized by surgery and rehabilitation with caliper. In polio residual deformity can be corrected by deformity corrective surgery, muscle weakness can be minimized by tendon transfer and strength training exercise, limb shortening can be minimized by limb lengthening procedure and rehabilitation by walking aid and caliper. With this measure their disability can be minimized by large extent and their capability can utilized in much better way.
Spina Bifida
Spina bifida is a developmental congenital disorder caused by the incomplete closing of the embryonicneural tube that lead to bony defect in vertebral canal through which the spinal cord and meninges may or may not protrude. If the anomaly is not visible, the condition is called spina bifida occulta. If there is an external protrusion of the saclike structure, the condition is called spina bifida cystica, and is further classified according to extent of neural involvement (e.g., meningocele, meningomyelocele or melomeningocele).
Spinal bifida occulta has only small defect in in vertebral column. Spinal column and nerve roots are usually normal
Meningocoele have the cyst which consist of memebrane of spinal card but spinal card and nerves are normal so cyst can be removed safely without affecting spinal cards and baby remain normal after surgery.
Meningomyelocoel is Most sever form of Spina bifida. In this problem The protruded portion of the spinal cord & the nerves which originate at that level of the cord are damaged or not properly developed. Extent of paralysis & loss of sensation depends upon the level of the spinal cord defect.
It present as swelling in midline of back as globular swelling anywhere from cervico-occpital junction to sacram. It can be diagnosed just after birth.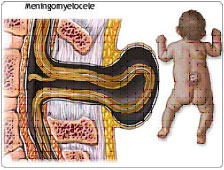
Management – Closure of defect required in early infancy. some time nerve fiber & part of spinal card are mal developed and adherent to the wall of cyst so there is always possibility of weakness in affected distribution. during surgery nerve and spinal card replaced in vertebral column defect coverd with skin and near by soft tissue. Then after surgery child referred for Proper assessment and evaluation of residual weakness and deformity. Prognosis depends upon spinal level of lesion & associated conditions. After complete evaluation child initially managed with proper positioning, splinting and therapy. In elder children when child develop residual deformity then multilevel orthopaedic surgical correction & tendon transfer supplemented with braces and caliper. Aim of treatment in these children to mobilize and make them ambulatory by any means. Aim of rehab is to prevent development of deformity in early age & Strength training exercise, reeducation of spared muscle & gait training with the help of orthotics and braces in later ages. Help of urologist are required to manage the problem of baldder disfunction. ifchild develop hydrocephalous then VP shunt is required to bypass CSF. With treatment child with spina bifida can became active individual.
Intoeing (feet point inwards)
It can be physiological or pathological. Normal at birth most of feet great toe is pointing inward that correct as age progress and becam normal around 10 year of age. But it may be pathological due to developmental problem like cerebral palsy, hip dysplasia, ricket. If it is pathological then pathology can be at hip joint (increase in anteversion of proximal femur), knee joint(knock knee). leg ( bowing) or in foot (metatarsal adductus ) itself.
The three typical causes of intoeing are: Metatarsus adductus (curved foot), Femoral anteversion (twisted thighbone), Tibial torsion (twisted shinbone)
Intoeing is common in newborn children, is usually the result of intrauterine positioning. metatarsus adductus occurs in one of 5,000 births and in one of 20 siblings of patients with metatarsus adductus. The incidence is higher in preterm children, multiple births and boys, and it occurs more often on the left. Strong association between metatarsus adductus & hip dysplasia found. The majority of these foot deformities will resolve spontaneously without treatment. Less than 5 percent of children will have a severe residual deformity at follow-up. Usually no treatment is required. On rare occasions, casting or special shoes might be required.
Dynamic forefoot addiction during walking is common in children up to age 24 months, due predominantly to increased activity in the abductor hallucis muscle. This dynamic great toe adduction occurs when balance and stability are improving. Spontaneous resolution without treatment is the norm. Surgery is rarely required
Femoral Anteversion
At birth, the proximal femur is internally rotated (anteversion ) an average of 40 degrees relative to the femoral shaft. As children approach age 8, anteversion diminishes to 10 to 15 degrees without treatment. As neonatal soft tissue contractures begin to resolve, the initial hip position of flexion and external rotation improves, and the thigh tends to internally rotate. As a result, intoeing due to retained neonatal femoral anteversion tends to become clinically evident as children begin to walk. Children with femoral anteversion usually sit in the W position. Running is often characterized by a windmill motion of the legs, because of the internal rotation of the thigh.
During the swing phase of gait (the portion of the gait cycle when the foot is off the ground). Intoeing is most noticeable between the ages of 2 and 5 years and gradually improves thereafter, up to age 12, as anteversion spontaneously improves.
Few children with persistent femoral anteversion experience functional difficulties in adulthood. There’s little evidence that femoral anteversion leads to hip arthritis. Rarely, intoeing in children older than 10 years leads to significant functional problems and requires femoral derotational osteotomy surgery. Typically, such children have internal hip rotation of more than 70 degrees and anteversion of at least 45 degrees.
Tibial Torsion – the most common cause of intoning in children 1 to 3 years old is internal tibial rotation. Parents of the majority of such children report that the children appear clumsy (fall and trip frequently). Parents often note that the children seem a bit bowlegged. In most cases, tibial torsion is bilateral. If unilateral, it’s more often noted on the left. Intrauterine molding is usually responsible. At birth, the average tibial internal rotation is 4 to 5 degrees (range -30 to +20 degrees). Spontaneous resolution occurs up to age 8 years. At maturity, the average bimalleolar axis allows 25 to 30 degrees of external rotation, and the thigh-foot axis allows 10 degrees of external rotation. Associated physiologic genu varum positioning is common, resolving when the child is about 24 months old.
Out toeing – Intoeing causes little functional difficulty in adults. Outtoeing, however, can be problematic because of tibial external rotation or excessive femoral retroversion, and it might be associated with more functional problems than intoeing is. Tibial external rotation might aggravate patellar tracking problems. Both tibial external rotation and increased external hip rotation might result in reduced pushoff power during walking and running. On occasion, formal gait analysis is necessary to evaluate such people, and surgical treatment might be necessary.
Flat Feet
Flat feet (the lack of an arch when standing) are common in all age groups. There are two types of flat feet, flexible and rigid. If an arch is present when standing “tip-toe” the flat foot is flexible. Flexible flat feet rarely produces symptoms or requires treatment. If an arch is not present when standing “tip-toe”, the flat foot may be “rigid”. Rigid flat feet are more likely to require further evaluation and possible treatment. Rigid flat feet are very -2 rare. Causes of Flexible flat feet may be physiological or due to some neuromuscular problem. And some time it may also be due to hyperlaxity. On other hand rigid flat feet are due to some joint pathology of talocalcaneal joint like inflammatory pathology or tarsal collision.
Treatment
Generally there is no treatment needed. However, a child with a painful flexible flat feet may benefit from soft arch supports. These provide only comfort and do not “create” an arch. Corrective shoes and bracing also do not “create” an arch.Flexible flat feet are a common, usually painless condition that is often normal. Corrective shoes or inserts do not “create” an arch. Flexible flat feet will not interfere with your child’s ability to learn to walk or play sports. Shoe salespersons may tell you expensive shoes will help your child walk better. This is not true. Regular, inexpensive shoes may be worn.
Article on cervical spondylosis
 Article on osteoporosis
Article on osteoporosis
Contact us
Call Us
0532-2468989
+ 91 9415014994
+ 91 8577873545
+ 91 9455001645
Email Us
totrishlaortho@gmail.com
Our Location
Dr. Jitendra Kumar Jain
Trishla Orthopedic Clinic & Rehab center, 182C / 350A, Tagore Town, Prayagraj (Allahabad) U.P-211002, India