Congenital Hip Dislocation Treatment
What is Congenital Hip Dislocation in Children:
Congenital hip dislocation is also known as developmental dysplasia of the hip (DDH) or hip dysplasia. It means that the hip joint in a newborn child does not develop fully, it may be just subluxation / dysplastic acetabulum or complete dislocation of joint. The hip is a kind of ball and socket joint. The hip joint is formed by the upper rounded end of the thigh bone & socket of the pelvic bone.
Causes of Congenital Hip Dislocation:
It is a congenital anomaly present since birth only. Most of the time causes are unknown but the breech presentation, less amniotic fluid in the uterus, and family history are the common causes. More common in a female child.
Symptoms of Congenital Hip Dislocation:
The symptom of congenital hip dislocation depends upon the age of the child at presentation. In newborns, the only unstable hip can be seen in the reducible hip but in the teratogenic hip, it may not be reducible. The hip joint will be completely dislocated so the affected thigh cannot be abducted and shortening of the limb. If both sides are affected then the distance between both lower limbs be decreases. A common symptom of CDH in walking age is painless limping, shortening, decrease in the abduction of limbs, abnormal gluteal fold, decrease range of motion at the affected hip joint. Diagnosis can be confirmed by clinical examination, an x-ray of the hip & pelvis, and ultrasound.
Risk Factors of Congenital Hip Dislocation:
Breech presentation, female sex, positive family history, firstborn, oligohydramnios, intrauterine position, and positive family history are important risk factors.
How to Diagnosed Congenital Hip Dislocation:
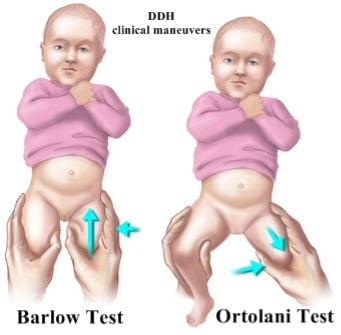
A congenital hip dislocation should be diagnosed as early as possible for the best possible care. It can be detected very easily within 6 months of age by a physical exam by the pediatric doctor. He can use the specific maneuvers to check the hip joint by listening to clicking/ clunking sounds that may indicate dislocation. This maneuver is known as Ortolani and Barlow test.
- During the Ortolanimaneuver, the doctor will try to reduce dislocated hip joint by pushing the hip inside and moving the thigh to outside.
- In the Barlow test, the doctor will try to dislocate the hip by taking the thigh inward and pushing the hip posteriorly.
Both this test is possible in very early before three months of age. After that, parents will complain of limb shortening, limping, inability to take the affected limb outside, and deep crease in the groin area. If both hips are affected, the child will have limping, lumbar lordosis, inability to sit cross leg, etc.
Initial investigation for diagnosis & confirmation of CDH is the ultrasound examination of the hip joint. By the ultrasound, we can see reducibility and degree of dislocation. But it needs an expert in doing that. X-ray of the pelvis with hip AP view is also needed to confirm the diagnosis of CDH. X-rays are being done in older babies. It also helps in identifying the acetabular dysplasia & extent of dislocation. MRI & CT Scan is rarely needed to evaluate cartilage status in very old children.


Congenital Hip Dislocation Treatment Options:
Congenital hip dislocation Treatment is started once diagnosis is being made. In infancy only Pavlik harness is required. It helps the child in holding hip join insitu. It is being wear by the child continues 24 hours in day for few months. But correct indication and reduciblilty will be decided by pediatric orthopedic surgeon in india. In some children, hip is not reducible in pavlik harness so these children may need close reduction & hip spica plaster. In children with teratogenic CDH, Early surgery to reduce the hip joint needed. Surgery is being contemplated once infant is fit for anesthesia but usually not before the age of six months. After 6 months of age, most of child need close reduction & hip spica plaster application. Child with CDH after the age of 1 year need open surgery to reduce the hip joint. Surgery will be followed by hip spica plaster application and brace for few months. Once child started walking, proximal femur goes up so they need shortening of femur bone and reconstruction of socket. Type of Congenital hip dislocation treatment is depends upon many factor and being decided by pediatric orthopedic surgeon after detail evaluation, considering the age, reducibility, grade of dysplasia etc.
How Congenital Hip Dislocation can be Prevented?
Congenital hip dislocation cannot be prevented but its complication can be prevented in long term if managed timely with good planning.
What are the Long Term Outcomes:
Early detection and early onset of congenital hip dislocation treatment give the best outcome. Whole hip joint growth is depends upon in-situ position of femoral head in acetabulam socket. So earliest placement of femoral head in well formed acetabular socket give excellent outcome. Delay in the surgery affect growth and development of acetabulam socket, femoral head and quality of smooth gliding surface of joint. One side hip dislocation can be operated upto any age with good outcome but in bilateral dislocation, results may not be good if delayed beyond 8 year age.
For More Information: Pediatric Orthopedic Treatment FAQs




Reference Links :
Frequently Asked Questions
Can a dislocated hip Be Fixed?
Yes, it can recover by good planning. In infancy by brace or plaster and after 1 year age child may need surgery. Normal recovery may take 4-6 months.
What happens if hip dysplasia is left untreated?
if hip dysplasia is left untreated, then it will cause pain, shortening, decreased function and ultimately result in hip osteoarthritis.
What exercises are good for Congenital Hip Dislocation?
Congenital hip dislocation need proper planning including reduction and surgery. Exercise have no role before reduction. Exercise need correct guidance.

Reviewed and Submitted by Dr. Jitendra Kumar Jain
Last updated on October 30, 2020
Dr.Jitendra Jain, MD and DNB (Orthopedics), president at Trishla Foundation, an NGO for treatment of cerebral palsy, and a Consultant Pediatric Orthopedic Surgeon & Cerebral Palsy Specialist at Trishla Orthopedic Clinic & Rehab Center.
Dr. J. K. Jain is a member of the general council at Dr. SMN university of rehabilitation, Lucknow, a member of the advisory board chief commissioner for PWD, Govt. of India (New Delhi), a member of the state disability research committee (U.P.), and a member of the committee of RCI, New Delhi. He has been awarded many awards, including the Dr.Bhagawan das memorial award, the spirit of humanity award, and the state govt. award for his services towards PWD, etc. Times of India has posted his work many times and mentioned him as one of the best doctors in the field of Pediatric Orthopedics. He helped many children recovering from cerebral palsy, just like comedian jay Chanikara, who is now able to stand and walk without any support, Abena, a Ghana girl with cerebral palsy, and many more. He also organized the National Wheelchair cricket tournament and created World’s first cerebral palsy village foundation in Prayagraj. He successfully treated 10,000+ children with various kinds of orthopedic disability, conducted 160+ free assessment camps, and produced a documentary film on cerebral palsy.
Walk in Appointments Available Daily
You can make an appointment online for video tale-consultation by fixing up an appointment at this website or you can visit the clinic to make an appointment in person and show to doctor with the care of social distancing at the given time.
Contact us
Call Us
0532-3550523
+ 91 9415014994
+ 91 8577873545
+ 91 9455001645
Email Us
totrishlaortho@gmail.com
Our Location
Dr. Jitendra Kumar Jain
Trishla Orthopedic Clinic & Rehab center, 182C / 350A, Tagore Town, Prayagraj (Allahabad) U.P-211002, India