Tibial Hemimelia
What is Tibial Hemimelia:
Tibia hemimelia is a rare congenital lower limb deficiency presenting with a wide spectrum of associated congenital anomalies, deficiency & duplication. It presents a wide range of pathology ranging from a hypoplastic tibia to a complete absence of the tibia. The fibula is always present, maybe normal, dysplastic, or duplicate. The incidence of tibial hemimelia is reported to be one per million live births.
Types of Tibial Hemimelia:
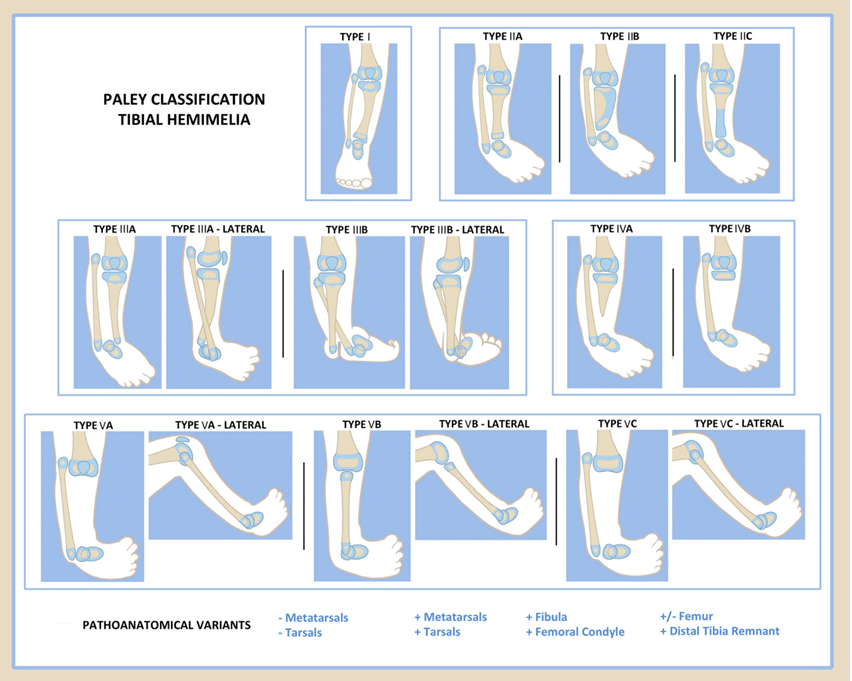
Tibia hemimelia has been classified by various experts worldwide according to anatomy, pathology, and treatment protocol. Jones classification was published in 1978. It was based on an X-ray finding. He divides into four types ranging from most deficient to least deficient. Then weber classification came. It was based on a scoring system so difficult to use in practice. We at Trishla Orthopedic clinic use the Paley classification system based on the severity of deficiency from least deficient to most deficient. This classification system has a direct relation with treatment & outcome.
- Paley type 1: Hypoplastic tibia: nearly normal tibia with genu valgum with relative overgrowth of the proximal fibula.
Also read: type-1-tibial-hemimelia
- Paley type 2: Proximal and distal tibial epiphysis present with dysplastic ankle.
- Type 2A: Well-formed distal tibial epiphysis & separate from proximal tibial epiphysis; tibial plafond present but dysplastic. Relative overgrowth of proximal fibula will be present.
- Type 2B: Delta tibia, proximal & distal growth plates connected through bracket epiphysis, mal-orientation of ankle and knee joints, ankle joint dysplastic, relative overgrowth of the fibula.
- Type 2C: Delayed ossification (cartilaginous anlage) of part, or all, of the tibia, dysplastic ankle joint, distal tibial epiphysis absent, relative overgrowth of the fibula.
Also read: type-2-tibial-hemimelia
- Paley type 3: Proximal tibia and knee joint present, medial malleolus present, distal tibial plafond absent, tibio-fibular diastasis present.
- Type 3A: Tibial plafond missing, medial and lateral malleolus present, varus diaphyseal bowing tibia, distal fibula (lateral malleolus) with foot internally rotated around the tibia, talus may be positioned between the tibia and fibula due to the absence of tibial plafond, relative fibular overgrowth.
- Type 3B: Same as 3A with skin cleft separating tibia and fibula, foot always follows the fibula.
Also read: type-3-tibial-hemimelia
- Paley type 4: Distal tibial aplasia
- Type 4A: knee joint present, the complete absence of distal tibia from the level of diaphysis pointed bone end often covered by separate skin pouch, relative overgrowth of the fibula.
- Type 4B: Epiphysis of proximal tibia present but absent proximal physis, knee joint present, delayed ossification of the epiphysis, relative overgrowth of the fibula.
Also read: type-4-tibial-hemimelia
- Paley type 5: Complete tibial aplasia
- Type 5A: Complete absence of tibia, patella present; flexion contracture of the knee, equino-varus contracture of dislocated foot and ankle
- Type 5B: Complete absence of tibia, no patella present; flexion contracture of the knee, auto-centralized fibula, quadriceps present, knee capsule present
- Type 5C: Complete absence of tibia, no patella present; flexion contracture of knee, dislocated fibula, quadriceps absent, no knee capsule present.
Also read: type-5-tibial-hemimelia
Causes of Tibial Hemimelia:
It is a congenital anomaly, present since birth. Genetic causes are the primary factor, otherwise, in most cases causes are unknown
Symptoms of Tibial Hemimelia:
Tibial Hemimelia can present in a variety of manner like from shortening to complete absence of tibia. Symptoms depend upon severity and type of tibial hemimelia. In the smaller tibia, the foot will be inward bend but as the severity of tibial deficiency increases, the grade of foot deformity increases. Few segments of toes can be absent along with severe equinus deformity of the ankle, fibula will be protruding beyond knee and ankle joint Child will not be able to bear weight on the affected limb, etc.
Tibial Hemimelia Treatment – Surgical & Non-Surgical:
In tibia hemimelia, the problem is in the main weight-bearing bone of the leg, so conservative treatment is not possible. Earlier, when we don’t have many options, In surgical treatment for tibial hemimelia, amputation & prosthetic feelings were the choices of treatment in tibial hemimelia. But now, with the work of Ilizarov and Paley, we can reconstruct most of the variety of tibial hemimelia. We follow the principle of Paley surgical technique in tibial hemimelia, so here we will give an outlook of Paley’s concept of treatment in this problem.
- Type 1: Limb lengthening of the tibia with correction of the valgus deformity.
- Type 2a: correction of equinovarus foot &tibial deformity by Ilizarov
- Type 2b: removal of extra cartilage from bracket epiphysis with correction of deformity and lengthening of the tibia by Ilizarov
- Type 2c: in this variety, delayed ossification of part or whole tibia is the present lengthening of the tibia with or without osteotomy of the fibula.
Bmp protein may be used for ossification of the tibia.
- Type 3 a: distraction of foot by Ilizarov, then reconstruction of ankle & deformity correction of the tibia.
- Type 3 b: distraction of foot by Ilizarov, then reconstruction of ankle & deformity correction of the tibia, repair between tibia & fibula syndesmosis.
- Type 4a: distraction of foot & knee by Ilizarov then tribalization of a fibula & tibiotalar arthrodesis.
- Type 4b: distal transfer of fibula and tibiofibular &tibiotalar arthrodesis.
- Type 5 a: reconstruction of the knee joint by utilizing patella (distraction of foot by Ilizarov, then reconstruction of ankle & deformity correction of the tibia)and fusion of fibular head to the tibiotalar patella arthrodesis.
- Type 5b: in this variety, knee disarticulation or knee reconstruction are two options. But this variety is very difficult to reconstruct.
How Tibial Hemimelia can be diagnosed:
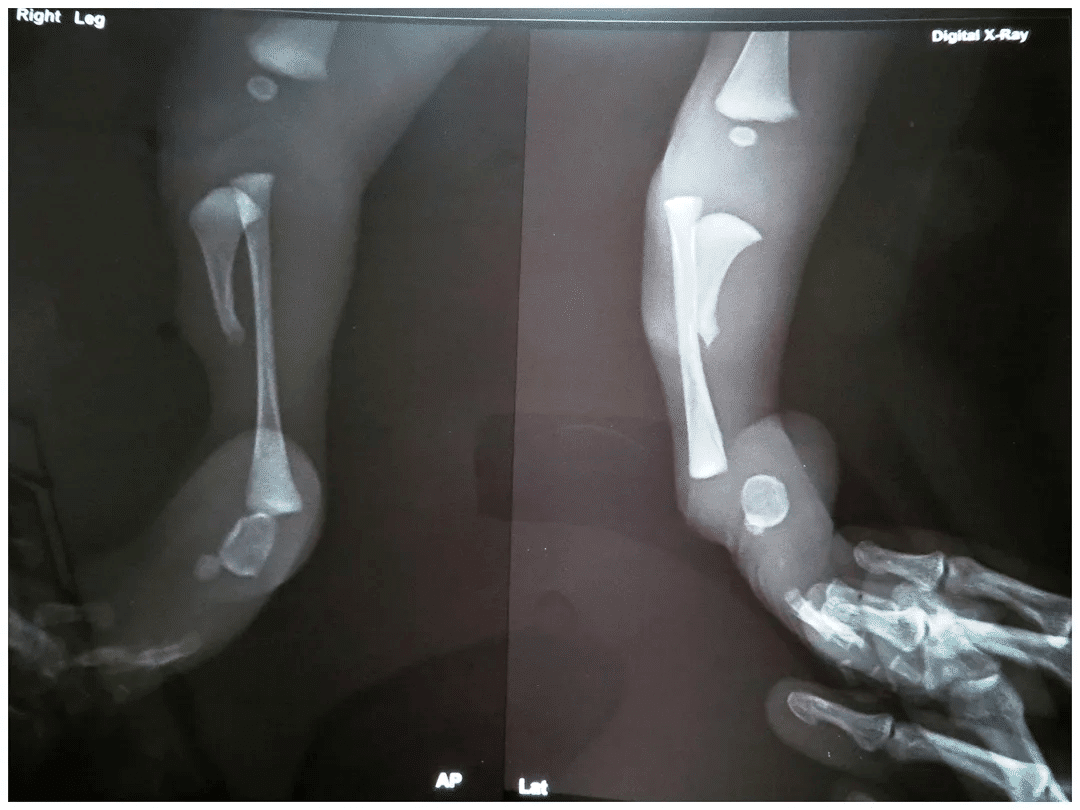
Tibial Hemimelia can be easily diagnosed by just looking at leg deformity at the time of birth but confirmation requires an X-ray of the leg.
Classification of Tibial Hemimelia:
Many classifications of Tibial Hemimelia has been done but Paley classification is most use full classification as per treatment protocol is concerned.
Tests needed for Tibial Hemimelia:
Sometimes it is also necessary to check another associated congenital anomaly so an X-ray of the whole extremity is needed. Some time MRI is needed to see an un-ossified tibial segment.
For More Information: Pediatric Orthopedic Treatment FAQs


Frequently Asked Questions
What are the causes of Tibial Hemimelia?
Tibial Hemimelia is a genetic abnormality. In most cases, the causes of this condition are not known also.
Which is longer tibia or fibula in tibial hemimelia?
Tibia is shorter or absent in tibial hemimelia. Tibia is weight bearing bone so surgery is must to maintain length of tibia.
What are the tests needed for Tibial Hemimelia?
- X-Ray
- MRI

Reviewed and Submitted by Dr. Jitendra Kumar Jain
Last updated on October 30, 2020
Dr.Jitendra Jain, MD and DNB (Orthopedics), president at Trishla Foundation, an NGO for treatment of cerebral palsy, and a Consultant Pediatric Orthopedic Surgeon & Cerebral Palsy Specialist at Trishla Orthopedic Clinic & Rehab Center.
Dr. J. K. Jain is a member of the general council at Dr. SMN university of rehabilitation, Lucknow, a member of the advisory board chief commissioner for PWD, Govt. of India (New Delhi), a member of the state disability research committee (U.P.), and a member of the committee of RCI, New Delhi. He has been awarded many awards, including the Dr.Bhagawan das memorial award, the spirit of humanity award, and the state govt. award for his services towards PWD, etc. Times of India has posted his work many times and mentioned him as one of the best doctors in the field of Pediatric Orthopedics. He helped many children recovering from cerebral palsy, just like comedian jay Chanikara, who is now able to stand and walk without any support, Abena, a Ghana girl with cerebral palsy, and many more. He also organized the National Wheelchair cricket tournament and created World’s first cerebral palsy village foundation in Prayagraj. He successfully treated 10,000+ children with various kinds of orthopedic disability, conducted 160+ free assessment camps, and produced a documentary film on cerebral palsy.
Walk in Appointments Available Daily
You can make an appointment online for video tale-consultation by fixing up an appointment at this website or you can visit the clinic to make an appointment in person and show to doctor with the care of social distancing at the given time.
Contact us
Call Us
0532-3550523
+ 91 9415014994
+ 91 8577873545
+ 91 9455001645
Email Us
totrishlaortho@gmail.com
Our Location
Dr. Jitendra Kumar Jain
Trishla Orthopedic Clinic & Rehab center, 182C / 350A, Tagore Town, Prayagraj (Allahabad) U.P-211002, India